Kawasaki disease is a rare inflammatory illness that primarily affects children under the age of 5. It causes inflammation in blood vessels throughout the body, and is one of the leading causes of acquired heart disease in children in developed countries. With early diagnosis and proper treatment, most children recover fully.
가와사키병이란 무엇인가요?
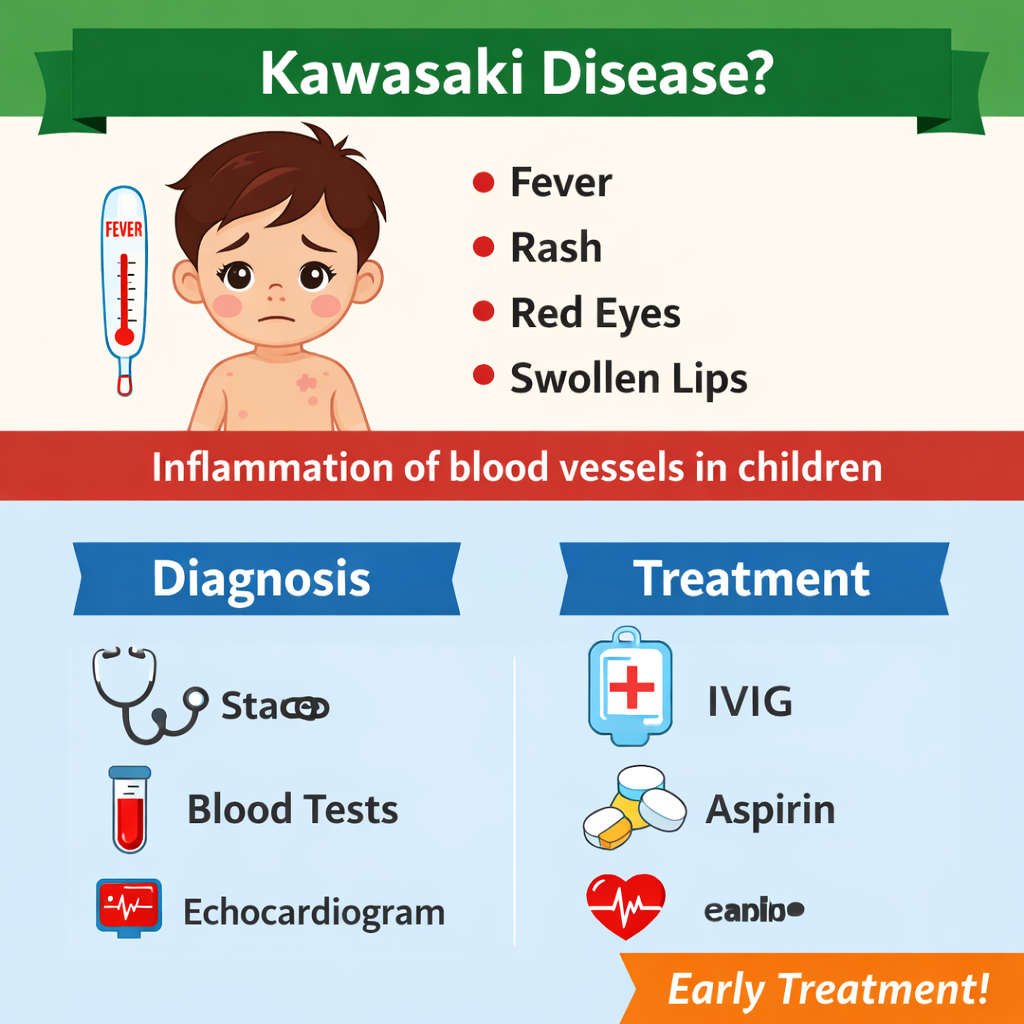
가와사키병은 주로 5세 미만의 영유아에게 발생하는 드문 급성 염증성 질환으로, 전신의 혈관에 염증을 일으키는 혈관염의 일종입니다. 특히 치료가 지연될 경우 심장 혈관(관상동맥)에 영향을 줄 수 있어, 선진국에서는 소아 후천성 심장 질환의 주요 원인 중 하나로 알려져 있습니다. 그러나 조기에 진단하여 적절한 치료를 받으면 대부분의 어린이는 심각한 합병증 없이 건강하게 회복할 수 있습니다.
More Specific Information: / 더 구체적인 정보:
Understanding Kawasaki Disease
Kawasaki disease, also known as mucocutaneous lymph node syndrome, was first described by Japanese pediatrician Dr. Tomisaku Kawasaki in 1967. It is characterized by prolonged fever and inflammation that can affect the heart, coronary arteries, blood vessels, skin, lymph nodes, and mucous membranes.
The disease is not contagious; you cannot “catch” it from another person. While the exact cause remains unknown, researchers believe it may be triggered by an abnormal immune response to an infection in children who are genetically predisposed.
가와사키병이해 요약
가와사키병은 1967년 일본의 소아과 의사 Tomisaku Kawasaki에 의해 처음 보고된 질환으로, 정식 명칭은 점막피부림프절증후군(Mucocutaneous Lymph Node Syndrome)입니다.
주로 영유아와 소아에게 발생하는 급성 전신 염증 질환으로, 지속적인 고열과 함께 몸 여러 부위에 염증이 나타나는 것이 특징입니다. 특히 심장과 관상동맥을 포함한 혈관, 피부, 림프절, 입안과 눈의 점막 등에 영향을 줄 수 있습니다.
가와사키병은 전염되는 질환이 아니며 사람 간에 전파되지 않습니다. 현재까지 정확한 원인은 밝혀지지 않았지만, 유전적 소인을 가진 아이에게 특정 감염이나 환경적 요인이 면역계의 과도한 반응을 일으켜 발생하는 것으로 추정되고 있습니다.
조기 진단과 적절한 치료는 심장 합병증의 위험을 줄이는 데 매우 중요합니다. 따라서 지속적인 고열과 의심 증상이 나타날 경우, 빠른 진료와 전문의의 평가가 필요합니다.
How to Recognize Kawasaki Disease
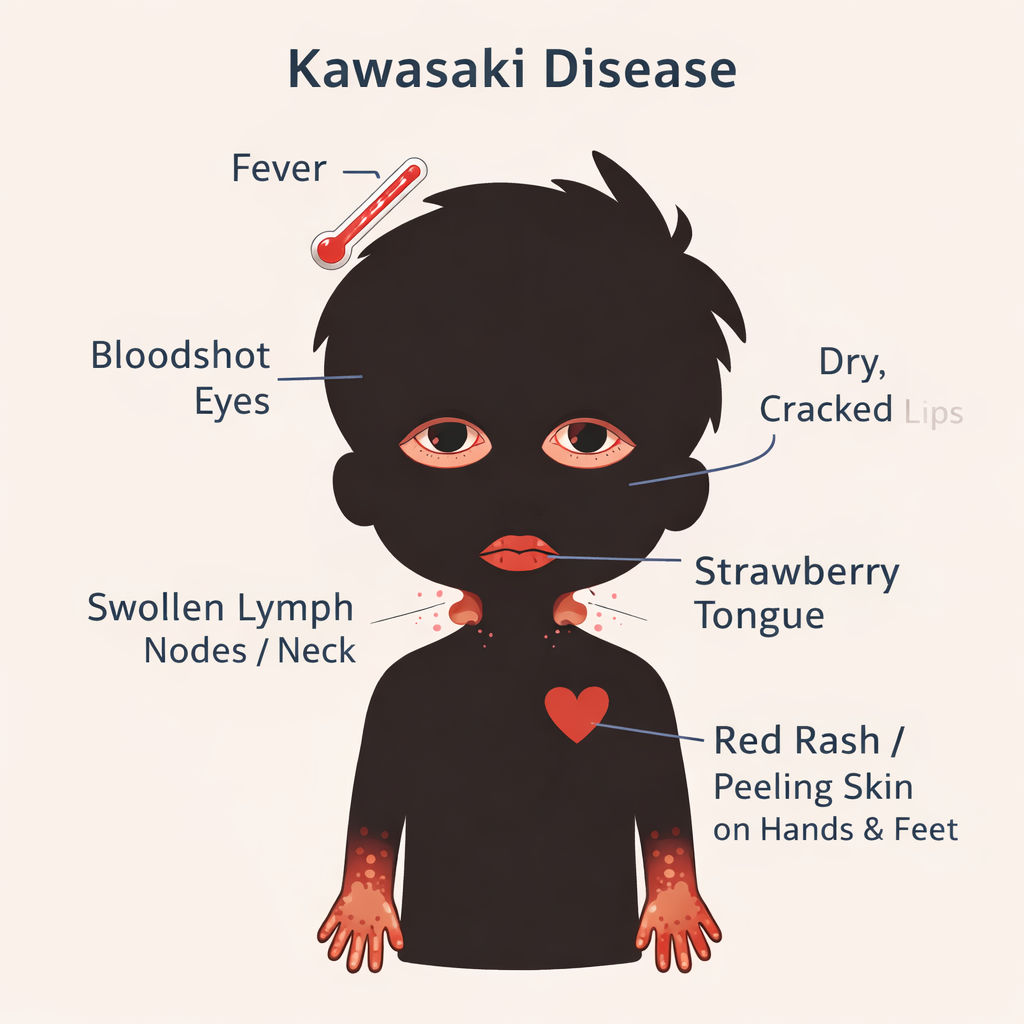
Doctors typically diagnose Kawasaki disease when a child has a high fever lasting 5 or more days, plus at least four of the following classic symptoms. Not all children display every symptom, making early recognition important.
High Fever: Persistent fever of 102–104°F (38.9–40°C) lasting 5 or more days, not easily reduced by standard medications.
Red Eyes (Conjunctivitis): Both eyes become red and bloodshot without discharge or crusting — called bilateral conjunctivitis.
“Strawberry” Tongue: Bright red, swollen tongue with prominent bumps. Lips may also be dry, cracked, and red.
Swollen Hands & Feet: Redness and swelling in the palms and soles. Skin may peel around the fingers and toes in later stages.
Body Rash: A widespread rash covering the torso and sometimes the genital areas.
Swollen Lymph Nodes: One or more swollen lymph nodes in the neck, typically measuring at least 1.5 cm in diameter.
가와사키병 인지 방법
지속적인 고열: 38.9~40°C(102~104°F)의 높은 열이 5일 이상 지속되며, 일반적인 해열제에 잘 반응하지 않을 수 있습니다.
결막 충혈(붉은 눈): 눈곱이나 분비물 없이 양쪽 눈이 붉게 충혈되는 증상이 나타날 수 있습니다.
딸기 혀 및 입술 변화: 혀가 붉고 부어오르며 표면의 돌기가 두드러지는 ‘딸기 혀’ 증상이 나타날 수 있습니다. 입술은 건조해지고 갈라지며 붉게 변할 수 있습니다.
손발의 붓기와 피부 변화: 손바닥과 발바닥이 붉어지고 붓는 증상이 나타나며, 회복 과정에서 손가락과 발가락 끝의 피부가 벗겨질 수 있습니다.
피부 발진: 몸통을 중심으로 다양한 형태의 발진이 나타날 수 있으며, 경우에 따라 생식기 주변까지 퍼질 수 있습니다.
림프절 부종: 주로 목 부위의 림프절이 붓고 커지며, 일반적으로 1.5cm 이상으로 만져질 수 있습니다.
가와사키병은 심장과 관상동맥에 영향을 줄 수 있는 질환이므로, 위와 같은 증상이 의심될 경우 가능한 한 빠르게 소아청소년과 전문의의 진료를 받는 것이 중요합니다.
The Three Phases
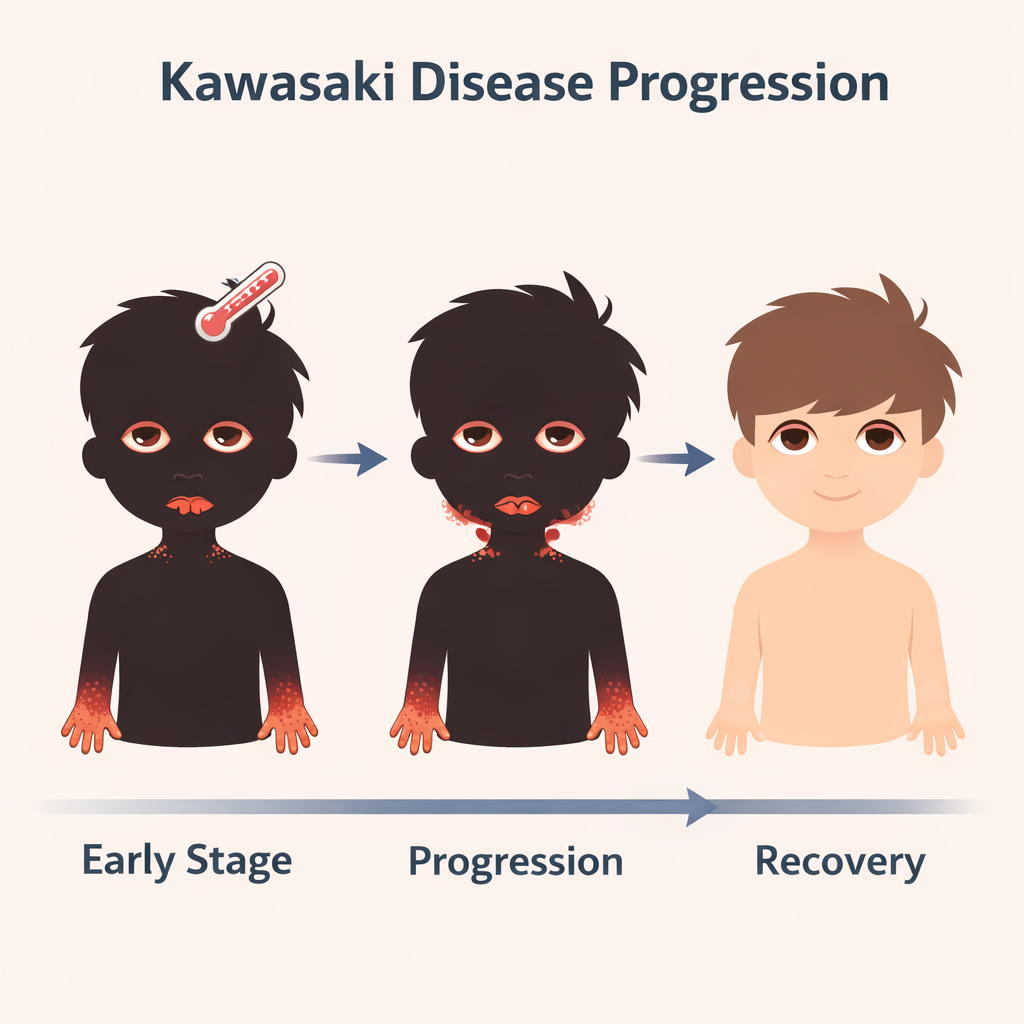
Kawasaki disease typically unfolds in three distinct phases. Understanding them helps families and caregivers know what to expect.
DAYS 1–14 · ACUTE PHASE
Onset of Symptoms: The most intense phase. High fever, rash, red eyes, and swollen lymph nodes appear. The inflammation of the heart muscle can begin here. This is when treatment is most critical.
DAYS 11–21 · SUBACUTE PHASE
Fever Subsides, Peeling Begins: The fever resolves, but skin on the fingers and toes may begin to peel. The risk of forming coronary artery aneurysms (weakening of artery walls) is highest during this phase.
WEEKS 4–8+ · CONVALESCENT PHASE
Recovery: All visible signs of illness disappear and blood markers return to normal. For most children, this phase ends in a full recovery. However, Kawasaki disease demands urgent attention due to its potential to cause serious heart complications. Without treatment, about 25% of KD patients will develop abnormalities of the coronary arteries.
*** If diagnosed and left untreated, it may cause blood clots and heart issues that will carry with you for the rest of your life.
가와사키병의 3단계
가와사키병은 일반적으로 세 단계의 경과를 보이며, 각 단계의 특징을 이해하면 증상의 변화와 합병증 위험 시기를 파악하는 데 도움이 됩니다.
DAYS 1–14 · 급성기 (Acute Phase)
증상이 시작되고 염증이 가장 심한 시기:
5일 이상 지속되는 고열, 발진, 눈 충혈, 입술 및 구강 점막 변화, 림프절 부종 등이 나타남. 전신 염증이 심장 근육과 혈관(특히 관상동맥)에 영향을 줄 수 있음. 조기 진단과 면역글로불린(IVIG) 치료가 가장 중요하고 긴급한 시기.
DAYS 11–21 · 아급성기 (Subacute Phase)
열은 줄어들지만 심장 합병증 위험이 높은 시기:
발열은 대부분 사라짐
손가락과 발가락 끝 피부가 벗겨질 수 있으며 혈소판 수치가 증가할 수 있음. 관상동맥류(관상동맥의 확장 또는 약화) 발생 위험이 가장 높은 시기. 심장초음파 등 지속적인 관찰이 매우 중요.
WEEKS 4–8+ · 회복기 (Convalescent Phase)
겉으로는 회복되지만 추적 관찰이 필요한 시기:
대부분의 외부 증상이 사라짐
염증 수치와 혈액 검사 결과가 점차 정상화됨. 대부분의 어린이는 완전히 회복. 다만 일부는 심장 혈관 변화가 남을 수 있어 정기적인 심장 추적 검사가 필요
중요: 가와사키병은 적절한 치료를 받지 않을 경우 일부 환자에서 관상동맥 이상이나 장기적인 심장 합병증이 발생할 수 있습니다. 따라서 조기 진단과 신속한 치료가 매우 중요합니다.
What Causes It?
The exact cause of Kawasaki disease is not yet known. Scientists believe it results from a combination of a genetic predisposition and an environmental trigger — possibly a viral or bacterial infection that sets off an abnormal immune response.
Who Is Most at Risk?
Kawasaki disease most commonly affects children under 5 years old, with boys slightly more likely to develop it than girls. It is more common in children of Asian and Pacific Islander descent, particularly Japanese and Korean children. It can affect children of all racial and ethnic backgrounds, however.
원인
가와사키병의 정확한 원인은 아직 밝혀지지 않았습니다. 현재까지의 연구에 따르면 유전적 소인과 환경적 요인이 함께 작용하여 발생하는 것으로 추정됩니다. 일부 바이러스 또는 세균 감염이 비정상적인 면역 반응을 유발하는 촉발 요인일 가능성이 제기되고 있습니다.
누가 가장 위험한가?
가와사키병은 주로 5세 미만의 영유아에게 가장 흔하게 발생하며, 남아에서 여아보다 약간 더 높은 발생률을 보입니다. 또한 아시아 및 태평양 지역 출신의 어린이, 특히 일본과 한국의 소아에서 더 높은 빈도로 보고됩니다.
그러나 가와사키병은 특정 인종이나 지역에만 국한된 질환은 아니며, 모든 인종과 민족의 어린이에게서 발생할 수 있습니다.
How Is It Treated?
There is no single test for Kawasaki disease. Doctors diagnose it based on symptoms and physical findings. Treatment for KD is available, and it must be given at the hospital. The goal for treatment is to lower fever, reduce swelling, and prevent heart damage. Treatment should begin as early as possible, ideally within the first 10 days of fever, to reduce the risk of heart complications.
• Intravenous Immunoglobulin (IVIG)
A high dose of IVIG is the primary treatment. It is given through a vein (IV) and helps reduce inflammation rapidly. Most children improve significantly within 24 hours.
• Aspirin Therapy non-steroidal anti-inflammatory drug (NSAID)
High-dose aspirin is used during the acute phase to reduce fever and inflammation. Lower doses are continued afterward to prevent blood clots, especially if coronary artery changes are detected.
• Cardiac Monitoring
An echocardiogram (heart ultrasound) is performed to check for coronary artery aneurysms. Follow-up echo appointments are typically scheduled weeks later.
• Hospital Care
Children are usually hospitalized during treatment for observation and to receive IV medications. Most are discharged within a few days once the fever resolves.
Note: Aspirin is not typically recommended for children due to the risk of Reye’s syndrome, a rare but serious condition affecting the brain and liver. Treatment for Kawasaki is a rare exception to the rule against aspirin use but only when given under medical supervision of your child’s doctor.
치료 방법?
가와사키병을 확진할 수 있는 단일 검사는 없습니다. 의사는 임상 증상과 신체 소견을 종합하여 진단합니다. 치료는 반드시 병원에서 이루어져야 하며, 주요 목표는 염증을 줄이고 발열을 조절하며 심장 합병증(특히 관상동맥 손상)을 예방하는 것입니다.
가장 효과적인 치료는 발열 시작 후 가능한 한 빨리, 이상적으로는 10일 이내에 시작하는 것입니다.
• 정맥 내 면역글로불린 (IVIG)
고용량 IVIG(면역글로불린)는 가와사키병의 핵심 치료입니다. 정맥 주사를 통해 투여되며, 염증 반응을 빠르게 줄이는 데 도움을 줍니다. 대부분의 어린이는 치료 후 24시간 이내에 발열과 증상이 크게 호전됩니다.
• 아스피린 치료 (비스테로이드성 항염증제, NSAID)
아스피린은 염증 감소 및 혈전 예방 목적으로 사용됩니다. 급성기에는 고용량으로 염증과 열을 조절하고, 이후에는 저용량으로 전환하여, 특히 관상동맥 이상이 있는 경우 혈전 형성을 예방합니다.
※ 일반적으로 아스피린은 소아에게 권장되지 않지만, 가와사키병 치료에서는 의사의 엄격한 감독 하에 예외적으로 사용됩니다. 이는 라이 증후군(Reye’s syndrome)의 위험을 고려하여 신중하게 처방됩니다.
• 심장 모니터링
관상동맥 이상 여부를 확인하기 위해 심장 초음파(에코카디오그램, echocardiogram)를 시행합니다. 필요에 따라 이후에도 정기적인 추적 검사가 진행됩니다.
• 입원 치료
대부분의 어린이는 초기 치료와 관찰을 위해 입원이 필요합니다. 정맥 주사 치료와 심장 상태 모니터링이 이루어지며, 상태가 안정되면 보통 며칠 내로 퇴원할 수 있습니다.